
Knowledge is power, and in the scene, knowledge is safety. For many in our community, age or health conditions bring new variables — specifically medications like Eliquis and Diltiazem. This guide outlines how to adapt your play to stay safe without losing the intensity.
One more thing before we start: everything in this guide assumes your play partner knows about your medications before the scene begins. That disclosure is not optional. It is the foundation everything else is built on.
1. Tell Your Top First
Before any technique, any positioning advice, any gear recommendation — your Top needs to know you are on anticoagulants, heart rate medications, or both. This is non-negotiable.
We know this conversation can feel awkward, especially early in a dynamic or with a new play partner. Here are a few ways to frame it during negotiation:
Ways to open the conversation:
|
A Top who is worth playing with will take this seriously. A Top who dismisses it is not a safe play partner, regardless of their skill level.
2. The Blood Thinner Factor (Eliquis / Apixaban)
When you are on an anticoagulant, your body’s ability to stop a leak is chemically inhibited. This changes the physics of impact play fundamentally.
- Hematoma Risk: What would be a light bruise for others can become a deep-tissue hematoma for you.
- Internal Bleeding: Heavy stingy or thuddy play can cause bleeding near organs or deep in muscle tissue that is not visible on the surface.
- The No-Fly Zone: Never take impact to the head, neck, or kidneys. On thinners, a head strike is a potential medical emergency — not a safety conversation, an ambulance conversation.
Note on dosage: The same medication at different dosages carries different risk profiles. Someone on 2.5mg twice daily is not in the same situation as someone on 5mg twice daily. Know your own dosage and share it with your Top. |
3. The Heart Rate Ceiling (Diltiazem / Calcium Channel Blockers)
Medications like Diltiazem are designed to keep your heart rate from spiking. In a scene, this creates a mismatch between your adrenaline response and your cardiovascular capacity.
- The Adrenaline Ceiling: You may hit a wall of fatigue or shortness of breath because your heart is being chemically held back while your nervous system is in full fight-or-flight mode.
- The Dizzy Drop: These medications make you prone to orthostatic hypotension — fainting when changing positions too quickly. Going from horizontal to vertical, or from kneeling to standing, can trigger a drop.
- Sub Drop Arrives Earlier: Because Diltiazem blunts the adrenaline response, the neurological crash after a scene may come sooner and feel more pronounced than players expect. Build in longer aftercare windows and communicate this to your Top in advance.
CRITICAL — When You Are on Both Medications If you are on both Eliquis and Diltiazem — common for AFib management — your risk profile compounds. A faint caused by Diltiazem leads to a fall, and a fall on Eliquis can lead to uncontrolled bleeding. This combination requires extra conservatism in positioning, extra vigilance from your Top, and ideally a conversation with your cardiologist before your next scene. |
4. A Note on Electro-Play and AFib
Sensory-focused play is often recommended as a lower-risk alternative when impact is off the table — and for many players on blood thinners, that is excellent advice. However, if you have AFib specifically, electro-play requires its own conversation with your cardiologist before you proceed.
Violet wands and similar surface-level devices are generally considered low-risk, but electrical stimulation and cardiac arrhythmia intersect in ways that vary by individual. Do not assume that because electro-play avoids bruising, it is automatically cleared for you. Ask your doctor directly.
5. Shifting the Style of Play
Stay Grounded
Prioritize on-the-deck play. Avoid suspension or high-post bondage where a fainting episode could result in a dangerous fall. This is especially important when Diltiazem is part of your regimen.
Shorten and Check In More Frequently
The adrenaline ceiling from Diltiazem means you may hit your limit faster than expected — and possibly before you feel it coming. Plan scenes to be shorter than usual. Build in explicit check-in points every 10 to 15 minutes rather than relying on safe words alone to signal when something is wrong.
Thud Over Sting
Avoid thin, high-velocity implements — canes, whips, small floggers. Use wide, flat implements that distribute force over a larger surface area to minimize capillary breakage and reduce hematoma risk.
The Power of Sensation
Shift focus to sensory play that provides a strong neurological experience with minimal physical trauma:
- Wax Play: Intense heat and weight sensation without bruising.
- Temperature Play: Ice and heat to engage the nervous system directly.
- Electro-Play (Violet Wands): Sharp, localized sensation without skin trauma — with the AFib caveat noted in Section 4.
6. Safe Word and Signal Considerations
If you are playing in restraints, gagged, or in positions where verbal communication is limited, your standard safe word system may not be sufficient given the additional risks above. Consider:
- A non-verbal safe signal (e.g., dropping a held object, tapping three times) that your Top has agreed to monitor.
- Checking in proactively at agreed intervals rather than waiting for a signal — particularly relevant with the orthostatic and sub-drop risks of Diltiazem.
- Making sure your Top knows the specific warning signs for your situation before the scene starts, not mid-scene.
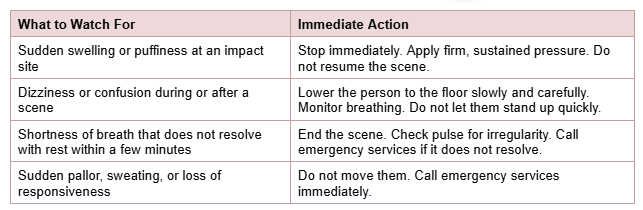
7. The Medical Protocol for Tops and Bottoms
Both sides of the dynamic should know what to watch for and what to do.
8. Scene Negotiation Checklist
Before any scene that involves physical intensity, both partners should have covered:
- Current medications by name and dosage — shared by the bottom, understood by the Top
- No-fly zones: body areas that are entirely off limits given the medication profile
- Positioning agreements: what positions are and are not safe given fall and fainting risk
- Check-in intervals agreed in advance, not left to chance
- Non-verbal safe signals confirmed and understood
- Aftercare plan that accounts for potential early or pronounced sub drop
A Note from Lady Leigh I have been teaching safety in this community for a long time. One of the things I have learned is that the players who ask the hard questions before a scene are almost always the ones who have the best scenes. Disclosing a medical condition to a play partner is not a weakness — it is exactly the kind of communication this community was built on. If you have questions about how your specific situation intersects with kink safety, reach out. That is what we are here for. |
Pro tip: When talking to your cardiologist, ask whether you can safely participate in high-contact sports like rugby. Their answer applies directly to intensity of impact play. It is a useful frame that gets you a clinical answer without requiring a longer explanation.
This guide is for educational purposes and reflects community safety standards developed through lived experience in the BDSM community. It does not constitute medical advice. Individual risk profiles vary based on dosage, overall health, and underlying condition. Always consult your cardiologist before engaging in physically or psychologically intense activity.

On staff at The LoftNC. Site webmaster and marketing assistant. Submissive, in a woman-led marriage that’s lasted over 25 years. Officially collared in 2023.